
Every risk is conclusively proven; every benefit needs further study.
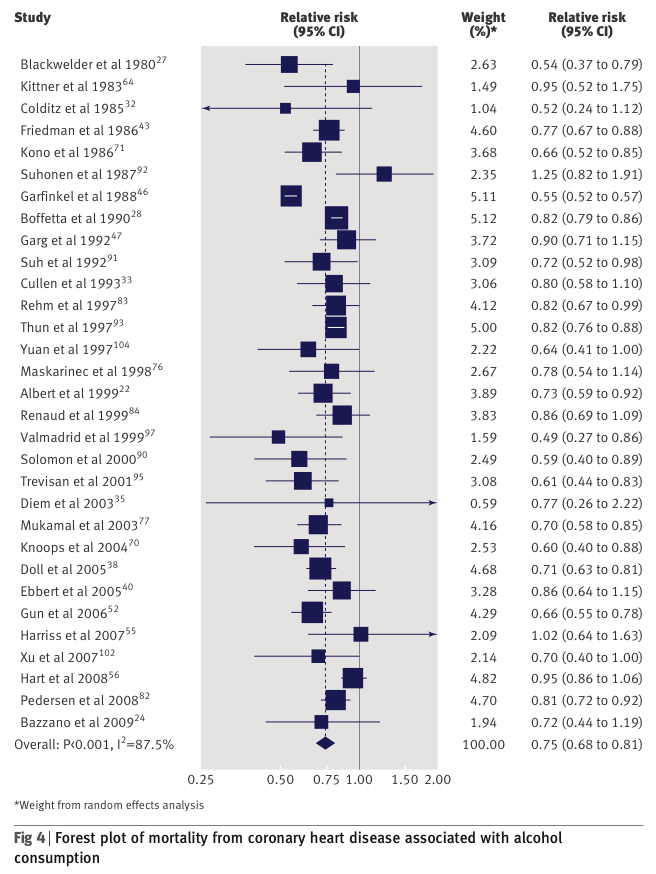
That's about the size of it. Of the benefits, there is research going back thirty years showing that the relationship between drinking and mortality is U-shaped or J-shaped, ie. risk is higher for total abstainers, lower for moderate drinkers and then rises again for heavy drinkers. This is largely the result of alcohol's protective effect on the heart. Reduced incidence of cardiovascular disease has been shown in many dozens of studies.
The correlations are consistent and (by modern epidemiological standards) fairly strong, but is there causation? If the popular media were any guide, you might think that the issue is shrouded in controversy. You may even believe that the J-shaped curve has been debunked.
The issue that is often raised is the "sick quitter" hypothesis—the idea that teetotallers are a sickly bunch who don't drink because they are chronically ill or because they have already destroyed their bodies with alcohol. In other words, alcohol doesn't protect health, it just so happens that teetotallers are unusually sickly.
David Nutt is a fan of this explanation, as are these Australians. I have seen Danny Dorling give this explanation on television. Ben Goldacre also uses it his book Bad Science (Unless it's for a Good Cause in Which Case I'll Look the Other Way):
Every time you read in a newspaper that 'moderate alcohol intake' is associated with some improved health outcome - less heart disease, less obesity, anything - you are almost certainly witnessing a journalist of limited intellect, overinterpreting a study with huge confounding variables.
This is because, let's be honest: teetotallers are abnormal. They're not like everyone else. They will almost certainly have a reason for not drinking, and it might be moral, or cultural, or perhaps even medical, but there's a serious risk that whatever is causing them to be teetotal might also have other effects on their health, confusing the relationship between their drinking habits and their health outcomes.
... Perhaps pre-existing ill health will force you to give up alcohol, and that's skewing the figures, making teetotallers look unhealthier than moderate drinkers. Perhaps these teetotallers are recovering alcoholics...
Well yes, perhaps they are. Who knows? If only someone would find out for sure...
Oh wait, they have. The "sick quitter" hypothesis was first put forward in 1988 and has been tested repeatedly in the last twenty years. The results of these studies showed that "sick quitters" do not explain the J-shaped curve.
Researchers have sought to address these concerns in several ways. Some epidemiological studies have separated former drinkers from long-term abstainers to address the sick quitter hypothesis. For example, in an analysis of 87,526 women, the risk of coronary heart disease was only 10 percent higher among former drinkers than among long-term abstainers (Stampfer et al. 1988).
Furthermore, the exclusion of former drinkers among the abstainers did not alter the 40 percent lower risk of coronary heart disease among women who drank 5.0–14.9 grams of alcohol (about 0.3–1 standard drinks) daily. Moreover, Rimm and colleagues (1991) found comparable risks of coronary heart disease among abstainers and light drinkers (i.e., people who consumed less than 5.0 grams of alcohol, or 0.3 standard drinks, daily) in their study of 51,529 healthy men, suggesting that abstainers are not an inappropriate reference group.
Other studies have excluded participants who developed coronary heart disease or died during the first few years of followup, as a means of excluding unidentified "sick" subjects, with similar results (Fuchs et al. 1995).
Taken together these findings indicate that the presence of sick quitters or former alcoholics among the abstainers is not responsible for the apparent benefits of alcohol consumption on the risk of coronary heart disease.
With other factors studied and discounted, the conclusion must be that alcohol has a protective effect on cardiovascular health. This, for example, from Rimm and Moats (2007):
A recent meta-analysis raised questions about systematic misclassification error in observational studies because of inclusion among “nondrinkers” of ex-drinkers and/or occasional drinkers. However, misclassification among a small percentage of nondrinkers cannot fully explain the inverse relation, and there is substantial evidence to refute the “sick quitter” hypothesis. Furthermore, it has been shown that moderate alcohol consumption reduces CHD and mortality in individuals with hypertension, diabetes, and existing CHD.
To address the issue of residual confounding by healthy lifestyle in drinkers, in a large prospective study we restricted analysis to only “healthy” men (who did not smoke, exercised, ate a good diet, and were not obese). Within this group, men who drank moderately had a relative risk for CHD of 0.38 (95% CI, 0.16–0.89) compared with abstainers, providing further evidence to support the hypothesis that the inverse association of alcohol to CHD is causal, and not confounded by healthy lifestyle behaviors.
Amongst those who studied the topic were Richard Doll and Richard Peto who concluded in 1997:
Thus, both in our study and in other studies that involved the observation of large numbers of deaths, confounding, in so far as it has been possible to test for it, does not seem to be responsible for the relatively higher vascular mortality in non-drinkers than in moderate drinkers. Hence we concur with the expert advisors to the European Office of the World Health Organization1141 that 'drinking modest amounts of alcoholic beverages is likely to reduce the risk of CHD [coronary heart disease] for some populations'.
Once of the more recent studies (Holahan et al., 2010) confirmed that alcohol's protective effect is independent of other factors.
Controlling only for age and gender, compared to moderate drinkers, abstainers had a more than 2 times increased mortality risk, heavy drinkers had 70% increased risk, and light drinkers had 23% increased risk. A model controlling for former problem drinking status, existing health problems, and key sociodemographic and social-behavioral factors, as well as for age and gender, substantially reduced the mortality effect for abstainers compared to moderate drinkers. However, even after adjusting for all covariates, abstainers and heavy drinkers continued to show increased mortality risks of 51 and 45%, respectively, compared to moderate drinkers.
This is what science is supposed to do. It asks questions of the data and tests plausible alternative explanations. The sick quitter hypothesis has been tested to death. It does not explain the J-shaped relationship between alcohol consumption and mortality.
Overall, even the most vociferous of critics agree that alcohol taken in light-to-moderate quantities, preferably regularly and with meals, appears to favourably affect ischaemic heart disease.
To ask questions of the data is right and fair. But to keep raising those questions after they have been answered makes me suspect you have an agenda. For some people, the potential of the sick quitter hypothesis to overturn the science was too good to be dropped even after it was disproved.
As Eric writes:
The modern literature (ie the last 4 years) seems to have thoroughly answered the critiques raised in the early 2000s about potential confounds in the J-curve. The worries about potential confounds were plausible: if "never drinkers" and "people who quit drinking because their health was terrible" were coded similarly in the data, that could produce a J-curve without any health benefits from moderate drinking. But that just wasn't what was going on in the data. It's been resolved.
Why won't this zombie argument lie down and die? The answer, I think, is that the temperance lobby hates the fact that total abstinence is not the optimal position and the public health establishment is always uncomfortable with nuanced advice. Advising moderation is fine for GPs, but politically active doctors and neo-prohibitionists prefer to frame things in terms of 'healthy' or 'unhealthy', 'good' or 'evil'.
I think it likely that within a few years the official advice will be to drink no alcohol at all. This would bring it in line with the World Health Organisation's absurd claim that there is no safe level of drinking.
The key message was that no safe level of drinking exists, so people should talk about levels of risk and drop terms such as “safe drinking”, “sensible drinking” and “alcohol misuse”.
This would be bad scientific advice and very probably bad medical advice, but what the hell? We can't have people seeing alcohol as anything other than an unmitigated evil can we?
As I recount in The Art of Suppression, American teetotallers scored a crucial victory when they persuaded the public that alcohol was a poison that could never be consumed in moderation. This was a lie then and it is a lie now, but it pathed the way for Prohibition. Moderation is the enemy of the zealous. Expect to hear much more about how the J-curve has been "debunked" in the years ahead.
Do have a read of Eric's blog posts on this topic:
The J-curve: science versus politics
Moderate drinking and health
12 comments:
Yes, Ben Goldacre is rather selective on the science he debunks.
In regard to cancer, rather than heart disease, the "sick quitter" principle has also been invoked. In recent years the article which has lent the most weight to the "no safe level" campaign is
http://jnci.oxfordjournals.org/content/101/5/296.abstract
http://jnci.oxfordjournals.org/content/101/5/296.full.pdf+html
by Allen et al. Below is a quote
"The increased risk seen in women who were currently nondrinkers
compared with light drinkers for many cancer sites suggests that
many nondrinkers may be former drinkers who have stopped
drinking due to illness, and this may have caused a spuriously high
relative risk in this group ( 48 ). Because of this, using current nondrinkers as the reference group category may not be appropriate and so nondrinkers were not included in out (sic) trend analyses of the association of the amount of alcohol consumed with cancer risk."
i.e. The left part of the J shape was removed. The accompanying editorial is here
http://jnci.oxfordjournals.org/content/101/5/282.full
Below is a quote
"Even if there are modest beneficial cardiovascular effects of alcohol, the current report of Allen et al. should remind us that we must consider these within a broader public health context. The current report, as well as a number of previous investigations, focused on middle-aged women. Among women, the major cause of death by far during the middle years is cancer (14). Although it is true that cardiovascular disease is the leading cause of death among women overall, this primarily applies to women older than 75 years. It might be reasonable to suspect that many women in the lay public who are asking physicians about any possible safe effects of alcohol are middle aged; for this large group, the only reasonable recommendation we can make is that there is no clear evidence that alcohol has medical benefits."
Professor David Spiegelhalter, on R4's More or Less, took issue with the authors' decision to remove the 250,000 non-drinkers from the million women in the study.
http://news.bbc.co.uk/1/hi/programmes/more_or_less/8040011.stm
All of the authors refused to take part in the the programme. A few weeks later, one of them was given a whole 25 minutes on R4 to spread, unchallenged, her anti alcohol message.
Very nice article Chris.I believe that pro-choice individuals and groups must embrace the 'everything in moderation' concept,versus the abstinence movement
That makes me wonder why even with smoking the same notion doesn't apply .Moderate smoking (i.e less than 10 cigarettes per day) is consistently shown in studies to be less harmful than heavy smoking and it must be comparable to other 'sinful' lifestyle choices (red meat,sugary food etc)
It would be nice if you put an article about it Chris
Ofcourse the approach from the medical establishment again is quit or die, on a crusade to find the holly grail and perhaps a couple of grants..
I think the mobilisation has begun and after a while a Framework similar to the one implemented for smoking will apply for Alcohol
http://www.euro.who.int/en/who-we-are/governance/regional-committee-for-europe/sixty-first-session/press-and-media/press-material/european-region-has-heaviest-drinking-in-the-world
But our good doctors have omitted dealing with the third leading cause of death (well at least in US)
http://jonrappoport.wordpress.com/2011/06/24/the-starfield-interview/
"Moderation is the enemy of the zealous."
Lol...What an understatement!
@karagiannis_dim
There is evidence to suggest that light - moderate smoking is beneficial to health.
The charts in the following link are interesting:
http://www.data-yard.net/science/therapeutic/wilsonphs.pdf
Interesting..thanks AuntieBan!
Lets look at just how big a problem CVD deaths is in the USA.
There are about 852,360 cvd deaths per 230 million adults per year.
That is a death rate of 37/10,000.
In any given year, 99.63% of the adults will NOT die from cvd.
A slight change, one way or the other, will have very little real impact on one's chances of cvd death.
This is a lot of crap about no real risk!
Gary K.
Epidemiology tends to involve lots of gormless, or dishonest, interpretation of correlation as cause. Consequently I tend to be highly sceptical of all purported results, even highly desirable ones such as the benefits of a wee drinky-pooh or a few squares of chocolate.
Moreover, I intend to enjoy my glass of red wine/white wine/beer/cider/whisky with lamb/fish/curry/pork/haggis come what may.
tudy: live to 100 by defying all health advice
Einstein College recently studied folks who lived past age 95. The reluctantly reported result: "People who live to 95 or older are no more virtuous than the rest of us in terms of their diet, exercise routine or smoking and drinking habits."
Einstein College press release:
http://www.einstein.yu.edu/home/news_pr ... 78&pt=news
Did you notice in link above that they just state that the very old smoked about as much as did people who died younger, with no detail given, although detail is given regarding eating, boozing, exercise, and so on? Well, when it came to publishing the abstract with the National Institutes of Health, they ignore smoking results entirely! They do say that smoking was studied, but make no mention whatsoever that smoking was not shown to impair longevity!
again, as with the press release, precise detail is given regarding other studied factors, but when it came to smoking -- the holy taboo of all holy taboos -- they simply couldn't bear even to mention their own finding!
Here it is: the official NIH abstract:
http://www.ncbi.nlm.nih.gov/pubmed/21812767
You'd probably have to pay about $50 to buy the full study from the Wiley service where it's posted. But you don't have to. A reporter for an independent publication who read the study tells us that about 74% of 70-year old men smoked and that smokers still made up the majority of over-95 men at 60%, while 26% of 70-year-old women smoked and a greater proportion of about 30% of over-95 women smoked, and that, all-in-all, the oldest folks did not particularly follow any of the Healthist advice to exercise, eat "healthy", or avoid booze and tobacco.
The news article:
http://lee-robinson-petzer.tumblr.com/p ... pectations
Did you note the researcher's conclusion: "Although this study demonstrates that centenarians can be obese, smoke and avoid exercise ... We should watch our weight, avoid smoking and be sure to exercise, since these activities have been shown to have great health benefits for the general population, including a longer lifespan."
cOURTESY OF KELLYNIUM AT SMOKERSCLUB,Reposted by harley
Given the evidence doesn't it follow that smoking bans would increase the CHD risks to both smokers and non smokers concerned with the effects of tobacco smoke. If CHD is the concern smokers should be encouraged to come back into the bars. Reducing their health risks with a beer and a smoke.
Post a Comment