
This is the "smoothed" graph presented by Pell in her study, which as noted in a previous post, does not even fit her own data. (The last 'year' shown is also not a full year.)
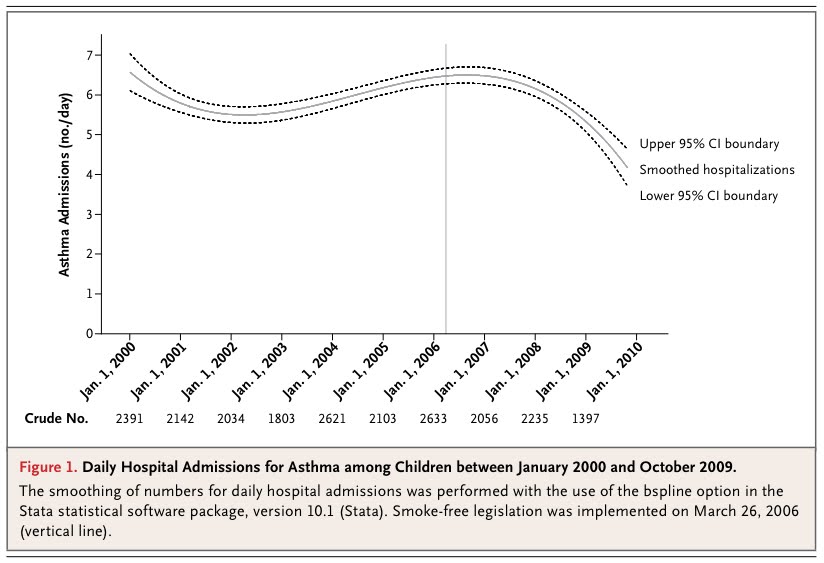
Pell's study produced the intended flood of media coverage, of which this Reuters report was typical.
Scottish smoking ban cuts childhood asthma attacksA 2006 public smoking ban in Scotland reduced the number of serious childhood asthma attacks by 18 percent per year, researchers reported on Wednesday.
Before the ban imposed in March 2006, the number of hospital admissions for asthma was rising by 5 percent a year among children under 15. The after-ban benefits were seen in both pre-school and school-age children.
Critics had said the ban could force smokers who could not light up in the workplace or in enclosed public spaces to smoke more at home, increasing the risk to children.
Dr. Jill Pell of the University of Glasgow, who worked on the new study, said the findings in the New England Journal of Medicine show that did not happen.
"The evidence we have from Scotland is that it had the opposite effect. People are generally more accepting of the need to protect nonsmokers and vulnerable groups such as children," Pell said in a telephone interview.
"Children were being exposed to less secondhand smoke. We went into the study hoping we would see some health benefit coming out of that."
However...
NHS Scotland has since published the statistics showing how many children were admitted to hospital with asthma between 2005 and 2009. These figures can be viewed here. They do not support Pell's hypothesis in any way, shape or form.
The graph below shows the rate of hospital admissions for asthma for children aged 0-14 years in all Scottish hospitals (per 100,000). The years shown are financial years (April to March - the first year shown is 2005/06), which is useful since the smoking ban was introduced in Scotland at the end of March 2006. Each of the last four bars therefore represent a full post-ban year.
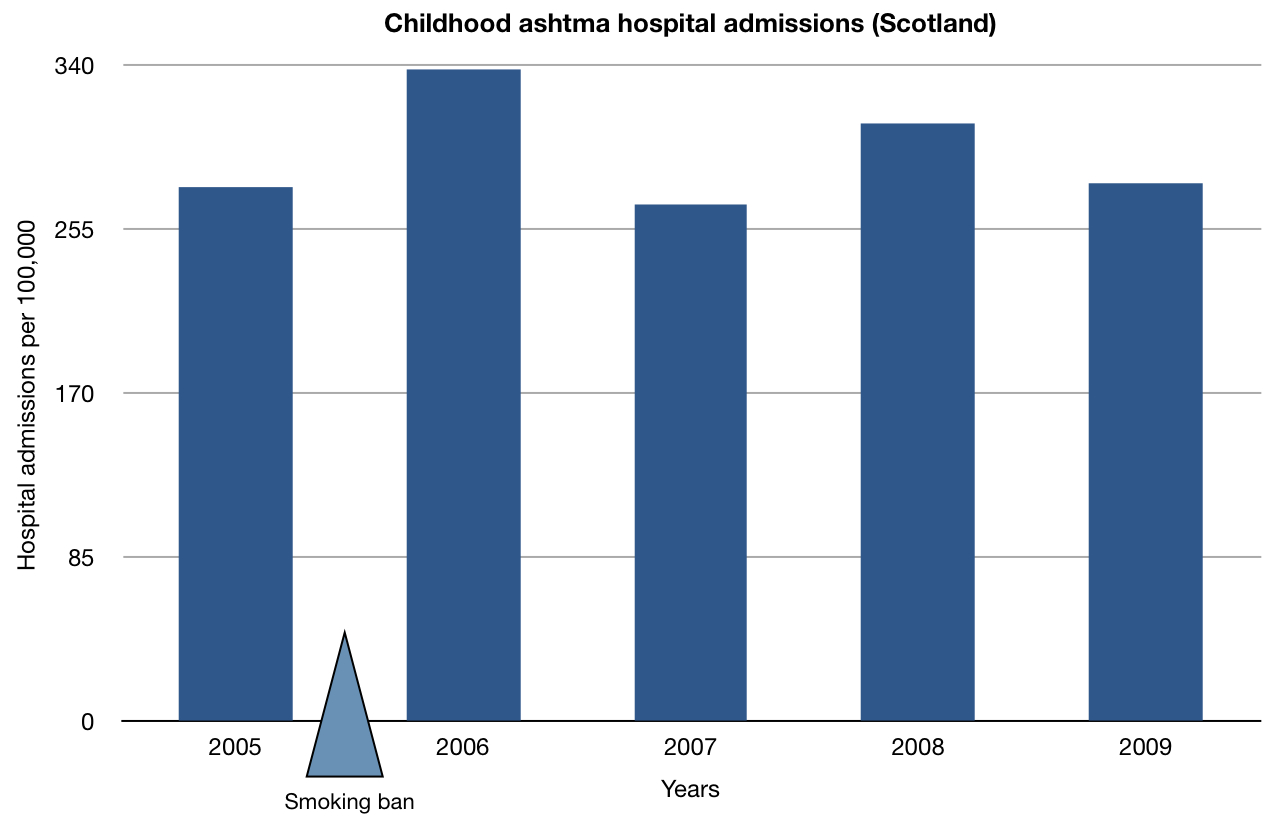
The next graph shows the total number of episodes of the same (ie. the absolute number of admissions). It naturally shows a very similar picture.


And, for good measure, let's have a look at hospital admissions for all diseases of the respiratory system combined.
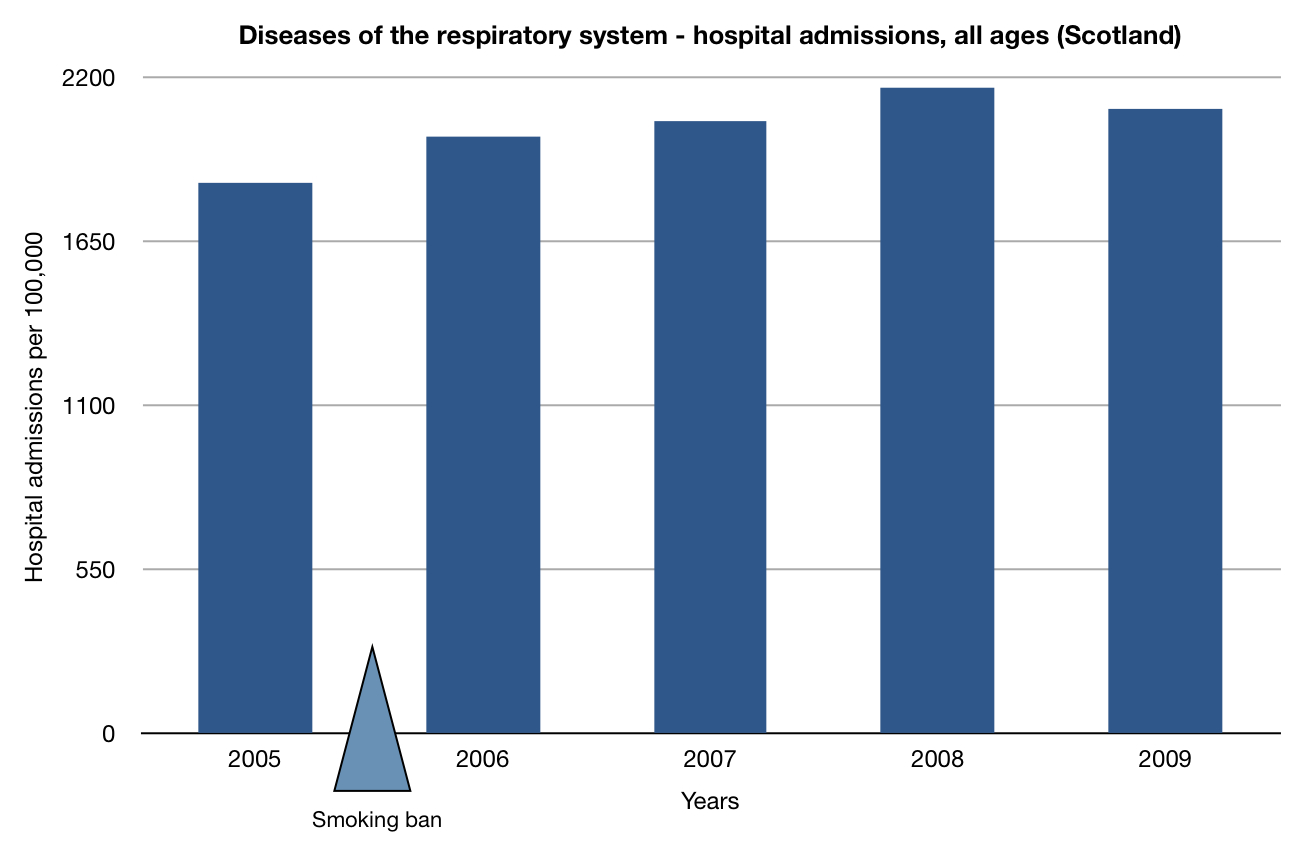
The data available online do not go back further than 2005/06 so we cannot see the long-term trend earlier in the decade. However, it is sufficient to see that there was no decline in hospital admissions for any of these diseases amongst any age group. If anything, there was an increase.
So, once again, you have a choice. You can choose to believe Jill Pell, a researcher who has, shall we say, "form" when it comes to producing studies like this.
Or you can believe the statistics produced by NHS Scotland which are based on the number of people who actually got admitted to hospital. These statistics, incidentally, support the claim made by Asthma UK that the rate of childhood asthma has remained essentially static for a decade.
It's your call.
11 comments:
Send the info to the NEJM (very prestigious)Editor and ask them to issue a statement about that paper being incorrect.
Send it to the NEJM - it will put them in a tricky situation; and send to Pell. Ask her to comment. She won't of course. Send it to R4 MoreorLess. They will be looking for ideas for their next series and they seem to like giving prohibitionists a kicking.
It is worth noting that Pell is a medic by training and so is the equally mendacious Anna Gilmore. Medics spend years learning how to fix sick people and I for one am deeply grateful for those who practice what they learn. I am less grateful for those who presume expertise in science and other disciplines in order to make a “contribution” to public health.
In addition, I cannot help but notice that much of the worst junk science seems to be published in “prestigious medical journals”.
Is there a theme worth developing here I wonder?
Just a thought.
I have yet to hear or see any of these people questioned over the data when being interviewed. They are allowed to spout forth, say whatever they wish and make any claim they want.
Is there a theme worth developing here I wonder?
I think it’s called agenda-driven, career-enhancing, industrial-partner-profiting FRAUD that is dictating public policy. And it is FRAUD because it is being peddled under the auspices of science and scholarship. This is not an isolated instance. The theme is that agenda-driven lying is rife and typically does not attract any critique within the PH® establishment: The bulk of them are reading from the same corrupt page. Peer review is hardly useful when the peers are similarly corrupt. Public Health® is seething with this ideological and profit-driven trash and opportunistic, fanatical, obsessed-with-control shysters.
To cut a long story short, I think there is a theme there. :)
Another triumph for Peer Review.
"I find it hard to imagine that a system this corrupt can be a good thing, or that it is worth the vast amounts of money spent on it."
Former editor of New England Journal of Medicine, Marcia Angell about the medical journals. Quote from her book:
http://www.amazon.com/dp/0375760946/
Have a look at the HES data for England. J45 and J46, same ISD classification as used by Pell et al, available here.
http://www.hesonline.nhs.uk/Ease/servlet/ContentServer?siteID=1937&categoryID=203
No noticeable trend either way as a result of the English ban, I'd say. Not for all patients, nor for U14s, not by admissions or episodes. Any attempt to extract any meaning out of this data is an attempt to sweat it far too hard in my view. There's just nothing there. Note that these are unadjusted for population change. That would make a slight difference, but nothing noticeable. As with the CHD figures, how strange that the same policy that changes the world in Scotland - according to Pell and co - should produce in England nothing noticeable.
There's a simple rule in stats that if your results look odd compared with the raw data, beware.
Sad, though maybe understandable given the nastiness they'd encounter, that almost no one in the stats or epidemiological professions seems inclined to police their own discipline for basic rigour on this issue. This is how science dies.
Here are some points for you.
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5745a3.htm
“The updated analysis indicated that, during 2000–2004, cigarette smoking and exposure to tobacco smoke resulted in at least 443,000 premature deaths, approximately 5.1 million YPLL, and $96.8 billion in productivity losses annually in the United States.”
Actually only 393,000 smokers’ deaths are used for the YPLL and productivity losses(wages).
The 393,000 deaths work out to be at an average age of 73.5, so over 1/2th of the people were retired and had no working income(wages) to lose as a cost to society.
About 9.1% of the smoker workers would be un-employed and would have no income to lose as a cost to society.
When a smoker worker dies, the job they were doing does not die with them. The employer will hire an un-employed worker to do the job and they will earn the wages the dead smoker is no longer earning.
There will be no loss of wages to society as they wages are still being earned.
The “$96.8 billion in productivity losses annually” is a crock of crap and mis-direction.
Gary K.
The lies have served their purpose (though how a ban in pubs was supposed to reduce children's asthma I am not sure). Now the actual stats will be used to ban smoking in cars and homes with children. Of course since it is impossible to tell which cars and homes will have children in them the bans will be comprehensive.
Off tangent but I am curious about the implications of this; I wonder if this article doesn't give us a glimpse of potential reasons for it.
After all this is a well established scientific fact.
Post a Comment